We’re past due for an update on #COVID19, aka Coronavirus and there is a lot to report/share.
For those who don’t know me, I am a career healthcare professional (senior care) who has been on weekly Coronavirus conference calls with Tx DSHS and regular CDC conference calls since the early stages of this pandemic. Working in senior care, my team has been hyper-focused on keeping our seniors completely safe and tracking the latest on this virus. My goal is to pass on the key points that we should all be focusing on.
I am concerned.
We had our weekly TDSHS call today (June 30th) and the tone was definitely one of greater worry. Dr. Jennifer Shuford (MD, MPH) who is the Infectious Disease Medical Officer for DSHS said they have been in bunker mode, working 7 days a week, tracking the spread in Texas. She noted they have been going so long it was hard to even track what day it was.
Add to that Dr. Anthony Fauci, Director of the National Institute of Infectious Diseases, noting on Tuesday that he is “very concerned” and believes that we could hit 100,000 new cases a day. To put that number in perspective, the highest we ever got when New York and New Jersey were at their worse was 31,992, on April 12th.
When a tsunami is coming, often the experts note it is coming, but those on the beach can’t see it and some – don’t believe it until it is too late.
The experts are waving red flags at us and we all need to pay attention. If you don’t believe Dr. Shuford and Dr. Fauci, note that as the 27 country bloc known as the European Union lifts its travel bans starting tomorrow, the United States is on the list of countries whose citizens are not allowed in, as the US is not deemed to have the virus “controlled”.
More and more of us are taking this seriously. Dr. Shuford and her team are asking us all to.
In this update, I am going to cover:
- The big picture
- Timelines for how COVID acts
- Economics
- Changes in how Texas and others will count cases
- What you can do to stay safe (yourself and others)
- At least one surprising insight on a long-standing vaccine that can help
The Big Picture
Ok, let’s start with the big picture:
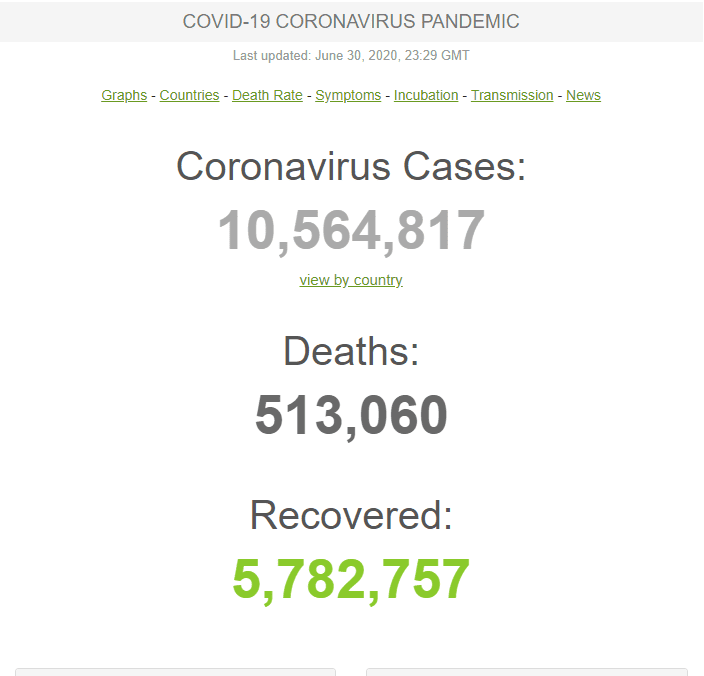
Total worldwide cases recently topped ten million cases and today sits at over 10,564,000 cases and over a half million deaths (513,060). So yes, this is very serious.
We need to remember we are in the midst of a global pandemic – the likes of which our country and our world has not seen in over 100 years. It is going to be bad for a while and the only way through this, is for us to materially change our behavior.
Let me pause here for a moment to say NONE OF US LIKE TO CHANGE OUR BEHAVIOR – I get that, I don’t either. And none of us like to be told what to do – I get that, I don’t either.
And we all know, sometimes we have to.
If we get a serious cancer, our life changes. Just like a serious cancer typically changes one’s lifestyle, is certainly a major threat and it screws up most everything – this worldwide pandemic is changing things for all of us.
Like a personal cancer diagnosis, those who take it seriously, become an expert on their cancer and learn how to deal with it/treat it/survive it. COVID-19 is impacting just about EVERYONE worldwide and we really, really need to follow the true experts’ advice. The evidence is there for us: countries that are taking the proven steps to contain this deadly virus are doing much better with limiting spread, limiting deaths AND they are going to be the winners economically.
Mask up, mask up, mask up.
By not masking up, we are putting our most vulnerable at great risk, now putting more healthy people at great risk and seriously threatening the economy and all of our livelihoods with it.
It seems like those who agree with the health risk are already taking it seriously and masking up. For those who don’t, recognize that whether you think this is overblown, a hoax, or something that we should let run its course – that a scared public doesn’t spend money, and if people don’t spend money, the economy crashes.
Why?
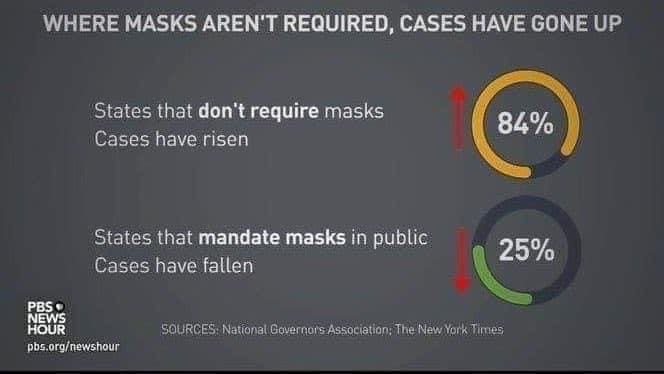
It is now clear that the countries that have masked up are doing much better in containing the virus, re-opening their economies and getting their citizens to buy and stave off economic disaster.
Is there some good news?
Is it still very dangerous and killing and severely injuring a lot of Americans? Also, yes.
The USA is unfortunately surging and now represents over half of the world’s cases at 2,724,693. So why did we open back up if it wasn’t safe? Well it is important to realize that opening back up did not mean we were past the risk, it meant we felt we were ready to handle the hospitalizations. And thus far we have handled the hospitalizations, although that may or may not last. But the experts advised citizens to take precautions when we re-opened and not enough of us did – and so numbers are increasing, and expected death projections are increasing.
The reality is that we took Coronavirus very serious in March/April and as a result, much of America didn’t see much happen. That wasn’t because it wasn’t a serious threat – it was because we shut down quite effectively. As a result, we all got a bad case of COVID-19 fatigue and we flunked the re-opening and now our nation’s death count today exceeded 130K with many more projected to come.
But while our nations cases account for over 50% of the world’s cases, our deaths only represent 25.4% of deaths worldwide.
So, is over half of the cases too much percentage wise? Yes.
Is 25% too much percentage wise? Yes.
With all of the resources and expertise we have, we should be doing much better, and many other countries are.
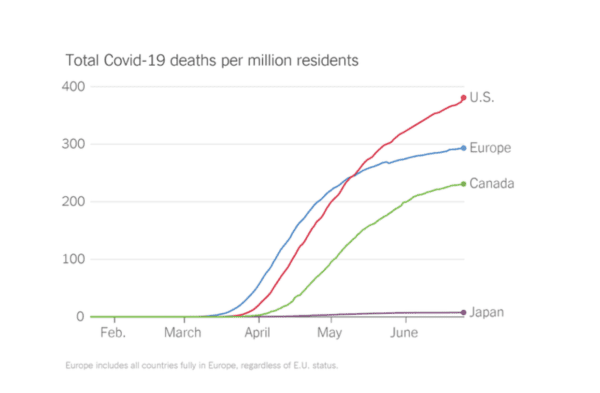
The US is obviously bigger than a lot of other countries so to truly compare apples to apples you compare cases and deaths per 1M in population. By that measure, in the US, for cases per 1M we are at 8,232 (and rising rapidly) and for deaths per 1M we are at 393 (and rising more slowly). By comparison, Brazil (another hot-spot) is at 6,596 (also rising rapidly) and 280 (rising more rapidly), Italy 3,979 (not rising) and 575 (also flat) and Sweden 6,778 (rising rapidly) and 528 (rising) on the high end and on the low end are countries/cities that did an outstanding job (and masked up) like Hong Kong at 161 and .9 and New Zealand 305 and 4. Hong Kong’s numbers are especially amazing given that they are very densely populated.
Two countries I didn’t cover were Belgium at 5,300 case per 1M and 841 deaths (really bad) and Madagascar at 80 cases per 1m and .7 deaths per 1m (amazingly good), because they have special circumstances related to MMR vaccination rates. More on that later.
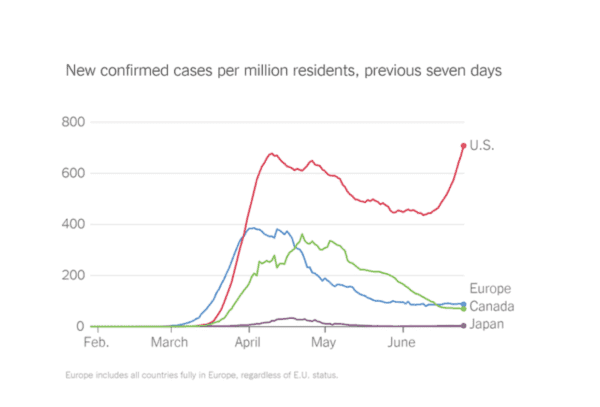
The big difference between us and most of the other poor performers is that we are surging (along with Brazil, India and Mexico), while most others are dropping. Experts say that we are going to have far more deaths than they predicted in April and absent a material change in behavior (masks/distance) it will likely get a lot worse before it gets better.
(Did I mention we need to start masking up?)
As noted, our previous peak as a country came on April 12th when we had 31,992 new cases in a single day before we started to drop.
Where are we now?
Well we have set new records for the last several days and are now adding new cases at a clip of well over 40,000/day, which is not good. So, our previous daily peak for cases was April 12th and our previous daily peak for deaths came on April 21st at 2,856 – 9 days after the daily caseload peak.
This leads to an important takeaway for us all, that being the time lags involved in COVID-19.
How COVID Data Trends Are Related
T0 = public change in behavior.
T + 2 weeks = change in new cases.
T + 2 to 4 weeks = change in hospitalizations
T + 4 to 6 weeks = change in death rates.
Said another way:
Whenever an area has a behavior change (getting better or worse at taking precautions) the case count changes (up or down) in about 2 weeks…
After a change in behavior, it takes 2 to 4 weeks before we see changes in hospitalization rates and 4 to 6 weeks before we see changes in death rates.
Here in Texas we are seeing surges in new cases (activities from 2 weeks ago), hospitalizations (activities from 2-4 weeks ago) and will likely see surges in deaths, in another 2 weeks.
Remember that America’s peak cases came on April 12th and peak deaths trailed 9 days later on April 21st, so as we set records every day this past week in America, expect deaths to rise in about 2 weeks.
Now the current surge is skewed more towards those under 65 so hopefully this round leads to fewer deaths – but if as expected, those middle aged and younger individuals carry they cases back to the elderly and those with co-morbidities (underlying conditions), we will see a secondary spike in deaths. Contract tracers (those who track how the virus spreads) note that most transmissions happen in the home, as one sick person infects the rest of their household. Bars and Parties are also high spread areas.
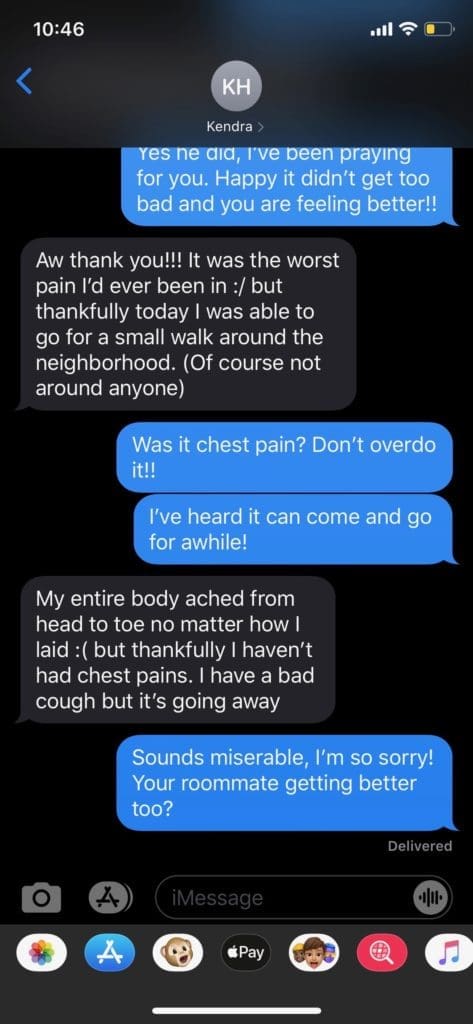
And remember a LOT of younger people are now landing in the hospital and those are called “moderate” cases. “Severe” means ICU. A “mild case” just means you weren’t hospitalized; it doesn’t mean you weren’t sicker than a dog. For many, a mild case means a miserable couple of weeks.
The below screenshot is regarding my son’s high school and college friend Kendra, a 21-year-old uber athletic and incredibly fit young lady with no underlying health conditions who noted it was the worst pain of her life.
Especially for those who aren’t as healthy as they once were, this is extremely dangerous. This is one of many reasons we have 24/7 nurses in our Assisted Living and Memory Care community (which is well above normal care levels). If a person with underlying conditions catches COVID-19, they are at far greater risk and need professional help.
So, back to the big picture:
- 48 of 50 states are seeing their numbers increase. Texas, Florida, Arizona, Georgia, South Carolina, Tennessee, Idaho and Utah are currently setting single day records for new cases. I can’t speak for those other states but given that some of our Texas hospitals are already getting uncomfortably high census in their ICU’s, the fact that another surge of hospitalizations is likely coming in the next week or two is not great news.
- In addition, when hospitals get hit with surges and have to restrict elective procedures, more people die of non-coronavirus deaths. If we can’t do biopsies, cancers spread, if we can’t do bypasses, more people die of heart-attacks, and on and on. So, when you don’t take this serious, get sick and take a hospital bed – even if you recover, you may be keeping the hospital from having the capacity for a critical elective procedure.
- The other concerning trend is the percentage of positive cases. “Total tests” is important, but what is more important for trending and analysis is the percentage of positive cases. Texas went from a positive case testing rate in the 4% range to now hitting 13%. That means a much higher percentage of those getting tested are positive which means that it is spreading rapidly in our communities and we have to change behaviors.
And trending is a key word – because we shouldn’t look at individual days, we should look at trends so we can predict where we are going, and the current trends are not good.
So what caused this spike?
Well let’s look back two weeks from when the spike happened (note graph) and you will see it coincides with the phases of re-opening the state. We have not succeeded in re-opening the state seemingly because we didn’t mask up and socially distance. It really is that simple – mask up/open up.

Dr. Santiago (who’s reporting on this has been outstanding) notes the following:
Since Phase I reopening in the DFW area, COVID cases are up 4.75 times (100% + 374% = 4.75X as large as the number of cases at Phase I reopening).
Since Phase II reopening, COVID cases in DFW have increased nearly 2.5 times (100% of original case load at Phase II reopening + 147% = 2.47X as large as the number of cases at Phase II reopening).
- We’re long past increases in case numbers being due to increased testing. (I deleted his comment about throat punching anyone who still claims this ?).
- D/FW is one of several major Texas areas having very large surges in COVID cases just in the last 2 weeks. Phase III reopening occurred after the surge started in Dallas/ Fort Worth, so expect many more.
- Deaths have been relatively low so far for Texas as an aggregate and in many cities compared to what happened in New York City and New Orleans. This is because the majority of new cases are in the 20-50 age group- COVID is spreading quickly through a younger age cohort that has less mortality. In Denton County (DFW area), about 40% of their new COVID cases are in the 20-50 age range. But INEVITABLY that age cohort will come into contact with age groups with have shown higher degrees of mortality in this pandemic.
- The absolute lack of public face mask use in Texas cities is adding significant fuel to this fire. Dr Joseph Chang MD (the chief medical officer of Parkland Hospital, the big county hospital for Dallas) mentioned it in his interview with WFAA three days ago. Masking is practically non-existent in many TX communities. I CANNOT STRESS ENOUGH THE VALUE IN PUBLIC MASK USE.
You should follow Dr. Santiago’s reports if you aren’t already doing so. He tags me in his posts every day and will accept your friend request if you want to follow him directly.
Texas is a hot spot and has now been designated an Endemic state (i.e. Endemic means our cases aren’t due to outsiders bringing cases in – this is because of insiders passing it around).
Our cases have risen so dramatically that earlier this week Governor Abbot had a press conference noting how serious things are turning, with Vice President Pence next to him and Dr. Birx on the other side and they implored Texans to please wear masks. Yep, the VP came to Texas to help stress the importance of masks.

Mask up, mask up, mask up. Mask up to open up.
The Economics
This is how we save lives. This is how we save the economy. This is really important.
And if we start masking up now, it will take 2 weeks for the case count to go down, 2-4 weeks for hospitalization rates to start to go down and 4-6 weeks for death rates to go down. And every day we don’t mask up is that many sicker, that many more dead and that much further that we batter an economy that experts worry can’t take much more.
You know the health risks but hear that the economic toll is devastating as well, and we must mask up now to keep it from getting worse.
But let’s pause a moment and discuss hospitalization and death rates.
When the virus first hit, it most heavily impacted the states with the greatest population density (NY, NJ, etc) and the frailest populations (nursing homes). As a country the experts were learning right with us, but now they have data.
Of the first 1,700,000 cases in the U.S., 14% were hospitalized and 2% ended up needing the ICU. 95% of those first 1.7M American cases survived, meaning 5% died.
5% died – let that sink in.
That is what the initial data shows, recognizing we didn’t have great testing capability so likely missed a lot of cases. Note only 5% of that first 1.7million were asymptomatic and in countries that have done better testing, they have found many more asymptomatic. So likely our total case count is higher (and death count) and our percentage of deaths is surely lower than 5%.
(Side note – we need extensive testing to accurately track and understand this virus.)
How Texas & Other States Are Counting Cases
Now let’s talk about how we get at the numbers.
Early on many people tried to compare Covid-19 to the flu, especially when death totals were in the 30-40 thousand range, as they would note that the flu killed 61,000 in a year. The problem is that flu deaths and COVID deaths were not counted the same way.
The CDC estimated the flu to have killed 61,000 in its worst year (2017/2018) and true average estimates over the last 10 years are about 2/3rds that (i.e. under 40K). But the key here is estimates – they truly don’t know how many people die from the flu, so they take death certificates that note the flu, and inflate that number to make up for under-reporting (i.e confirmed flu deaths are much lower than the reported/estimate deaths).
Early on in the Coronavirus pandemic, America reported only confirmed COVID-19 cases and yet the experts knew that was underreporting actual cases, as many who got it, and many who got it and died were never tested.
So, in April, the CDC rolled out new guidelines to capture estimated cases in addition to confirmed in the hopes of capturing more accurate data. Like all estimates, there is no way to prove the accuracy of these numbers – one has to trust the expertise of those making the estimates. NY had a one-time jump in cases, once they adopted this new measure to catch up what they felt were previously missed cases.
So why am I bringing this up now? Well it was up to each state on whether they adopted the new reporting guidelines and Texas just now agreed to adopt it. So now TDSHS may or may not be tallying the cases and taking that over from the counties. If they do, the new way of counting will include confirmed and expected cases and could materially bump up our numbers. Some are concerned that adding expected cases will lead to case inflation, covering those with the symptoms due to an unrelated illness and others are saying “finally” we can count the people we are certain have it, but we can’t get them tested.
Here are Collin County leaders discussing it (15ish minute mark) and their concerns.
So, I asked about it on today’s TDSHS call and they noted they are not at this time switching their reporting mechanisms or taking that over from the counties. If they do, it feels like we will go from a system that likely underreported to one that could now over-report. I have one doctor friend who is not happy with this change, fearing case inflation and one who thinks it is long overdue (and will be more accurate).
That said, the State has not yet changed how it reports cases, so recognize the current spike in cases is actual test confirmed cases. And regardless, hospitalization numbers are increasing materially – and at the end of the day, hospitalization and deaths are truly the numbers that count. Expect the new way of counting overall cases to start in the next week or so.
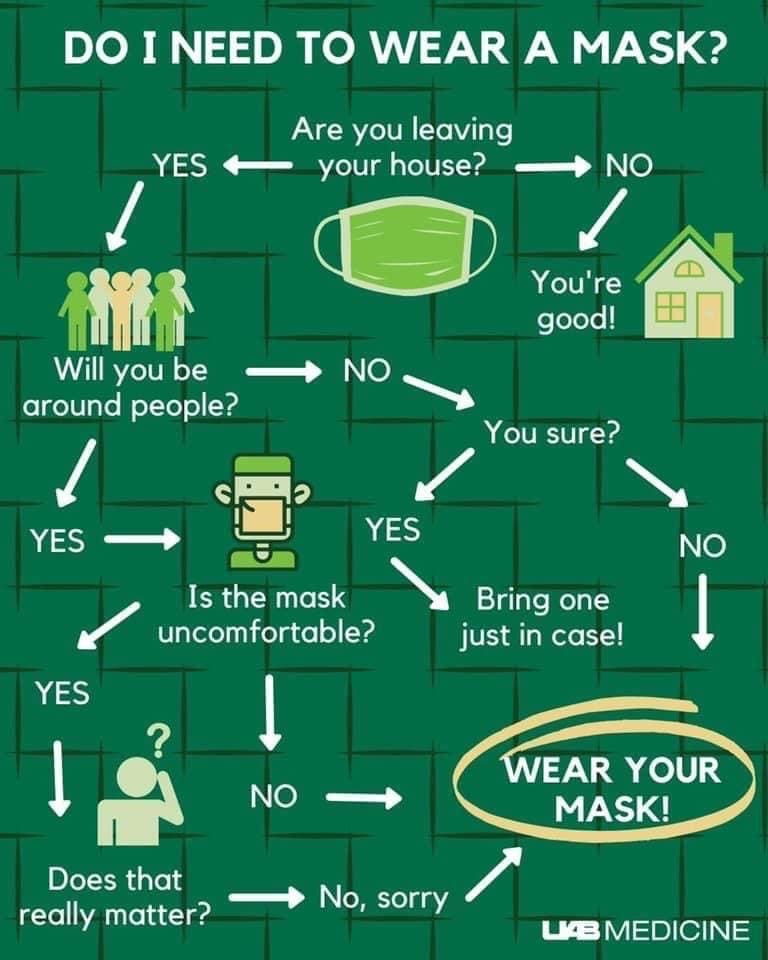
What Can You Do to Stay Safe?
Well let’s start with the easy stuff: Mask up. That alone would make the biggest difference.
And no, you won’t breathe in your own carbon dioxide and get dizzy or die as a result. If that were the case, surgeons couldn’t perform 8+ hour surgeries with masks on, construction workers couldn’t do lengthy demo work and none of the healthcare workers in our ICU’s could perform their jobs.
Yes, you could experience claustrophobia (I did) but with a little practice wearing it at home, before you go out, you can do it.
But don’t take my word on it, follow Dr. Hance, another true expert on the subject (who does a great job of citing her sources as well):
Will Americans be safer if we mask up? Judge for yourself. Here is the difference in deaths between now and Oct 1, if we do nothing and if we mask up.
Said another way: a LOT more Americans will die, and the economy will suffer a lot more if we don’t mask up.
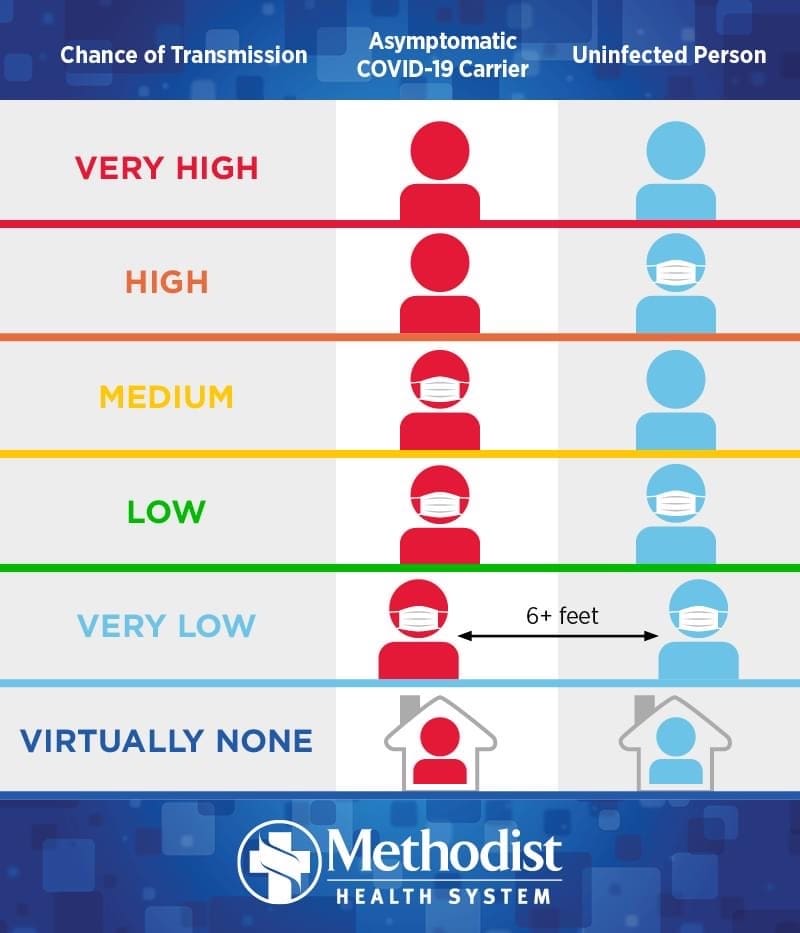
A friend who leads a very large senior care community did a full test of all of her staff and found one person was infected – and yet they hadn’t passed it on to a single person (co-worker or resident).
Why? Because she insisted everyone wear masks. Yes – masks do dramatically lessen the risk of passing it on, especially if you (like this staff member) don’t know you are sick.
So, WEAR MASKS.
And to be extra safe, wear eye protection. The primary transmission points for a respiratory droplets virus are your mouth, nose and eyes (tear ducts). Face shields are both an effective and more comfortable way to protect yourself – I have ordered them for all of my staff, but they don’t replace a mask.

Socially distance – 6 feet is the stated rule. (Virus in a normal conversation typically travels 4ish feet but a sneeze or a cough can cover 2 meters+ (6.5 feet), so stick 6ish feet away, because you never know when someone will cough.
And consider getting an MMR booster. Yes, an MMR booster – my wife and I got ours Tuesday. It has not been fully vetted as a treatment, but countries with the highest vaccine rates (and most recent ones) for MMR are doing MUCH better against COVID-19.
Compare Madagascar, a country of more than 25 million citizens that has only had 16 deaths to date. WOW. And now look at Belgium a country with 11.4 million citizens that is approaching 10,000 deaths. The difference – MMR vaccination. Massive difference between the countries in their rates of vaccination and how recently they had them done/boosted them.
Here’s Dr. Hance’s explanation
Here’s CNN’s Health’s explanation.
So, what else is out there?
Let me end with two things – UV lighting and how most folks catch this.
You may remember the hubbub about UV lighting. Well it really does kill the virus, which is why we installed it in the ventilation systems of our Teresa’s House – Craig Ranch Assisted Living and Memory Care Community. It is also why hospitals have used it in operating rooms for years to keep a sterile environment. I would encourage any business to install it as a proven safeguard for all. But you don’t want to look at it or have it contact your skin (think a really bad sunburn). It should clean the air but not be near you – which is why it is perfect for ventilation systems.
And that leads me to my final thoughts. Ventilation systems are where we focused much of our safety measures in the design of our Teresa’s House senior care community – because breathing this virus in is where you have your greatest risk.
At the end of the day, it is all about protecting your lungs as this is passed on through respiratory droplets. I have covered masks (for you and hopefully those around you) but also remind you to stay out of small, poorly ventilated spaces with other people.
Limit the time you are near others. The experts consider a non-healthcare “exposure” to be about 15 minutes within 6 feet of someone. But that assumes someone is talking at a normal tone of voice. If they shout (sporting events), sing (choirs), laughing sneeze or cough, you can get a big enough dose of the virus in a much shorter time, and in the case of a cough/sneeze, in an instant. Even a loud talker is a danger because the virus typically rests in your lower lungs so anything that forces more air out of your lungs, brings more virus with it. Even being outside won’t protect you if you are face to face with someone who is shouting, singing, laughing, coughing, sneezing or even talking directly at you if they are close enough and for enough time.
So, wear your mask, get outside, get your MMR booster and make sure wherever you go, there is good ventilation and you can socially distance.
Last thing – go easy on the experts for early misses. This was a new virus (novel means new), first seen in 2019 (thus the name Covid-19) and it has not acted like other viruses. There were some early mistakes, but they are now pretty dialed in and we need to take their guidance. We are seeing that not taking effective precautions was a mistake and the quicker we start taking those precautions (masks) the quicker we return to as close to normal as one can in a pandemic.
Don’t live in fear – but do show due respect. This virus is deadly to some and dangerous to most all.
Feel free to share.
And wear your masks….











































